Blog
To the Apex-Endodontic Blog for General Dentists
Sign up with your email address to receive news and updates.
Contact Us
2TheApex: AAE Guide RIGHT HERE! ADA Guides here! Key points to note: Antibiotic inadvertently NOT administered pre-operatively can be given up to two hours following treatment.If the patient is already taking an antibiotic, a different class antibiotic should be given for prophylaxis. (Example: Patient already taking Penicillin for days is not good enough and should be given another class of antibiotic acceptable for prophylaxis, i.e. Clindamycin 600mg)In general, NOT recommended for prosthetic joint implants unless specifically prescribed by the patient's orthopedic surgeon. Their surgeon should recommend the specific regimen and ideally write the RX for the patient when possible.(image: Staph. Aureus)

2TheApex: Yes. Pulpotomies are a good way to get a patient with irreversible pulpitis some relief until root canal therapy can be fully completed. Profound anesthesia is key. After popping into the pulp camber change your bur to a non-endcutting bur like the Endo-Z bur . Run the bur around the chamber and remove any tissue above the canals. Do not be temped to use any files in the canals. Staying out of the canals is key to a pulpotomy. Pressure with a hypochlorite soaked pellet usually stops any bleeding. Rinse the chamber with hypochlorite, dry and restore with a cotton pellet and temporary restoration. The insurance code for the procedure is D3220 Endo Emergency procedures reference

2TheApex: Asymptomatic vital tooth, isolation, coronal seal, and a bio compatible material are the keys to a direct pulp cap. Tooth status: Asymptomatic carious exposure or recent trauma, no history of symptoms suggesting irreversible pulpits, and an an incompletely formed apex. Pulp testing should be done prior to anesthesia. Prognosis of a direct pulp cap from a carious exposure in a mature tooth is very poor and often leads to more problems in the future. Isolation: Rubber dam isolation is very important, saliva contamination will cause bacteria to be introduced to the site. NaOCl soaked cotton pellet should placed gently but firmly on the exposed pulp to decontaminate the area and control bleeding. Persistent and excessive bleeding is a sign of inflammation and likely irreversible pulpitits. A pulp cap should not be attempted in this situation. Bio compatible material: MTA or other bioceramic material is the preferred. Traditionally CaOH has been used, however this is less biocompatible and will eventually break down. Seal: The seal is the deal! Coronal leakage will invariably lead to pulpal pathosis. We recommend placing thin layer of Vitrebond directly over the pulp cap material, then proceed with a bonded final restoration immediately. Manage expectations: Inform patient of the possibility that root canal treatment may still be necessary.
2TheApex: Bilateral Nerve blocks were more successful (38% Uni- vs. 64% for Bilateral) Mandibular teeth with Irreversible Pulpitis are the most challenging to gain profound anesthesia. Due to some cross-innervations depositing anesthetic at BOTH mental foramina was found to be more successful that just one. Of course a Mental Nerve block may be preferred by patients since the tongue is not numb and it has a faster onset of action than an inferior alveolar nerve block. Reference Click Here
All of this is so rapidly changing our thoughts may change tomorrow. Dated 3/15/20 DETAILED ARTICLE IN NATURE The above article has detailed screening questions. ADA INFO Our door sign More info will be posted once we get our protocol together. Please share what you and your office is doing. Thank you, Derek Thanks Dr. Clara Ping for tip on Nature article

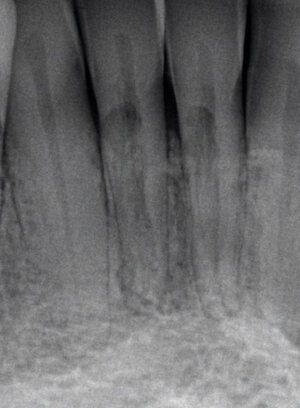
2TheApex: There is no cut and dry answer for cracked teeth. The decision to extract or save a tooth should be based on a through clinical evaluation and a discussion with the patient about prognosis, risks, benefits, and alternative treatment options. Cracked teeth (not to be confused with split teeth or vertical root fractures) are a challenging topic to discuss with patients. Below is a small checklist that we use to run through decision making with the patient when deciding to save or extract a tooth. 1) What does the patient want? Are they willing to take the risk of the tooth having a short life span even with root canal treatment and crown placement? 2) Systemic factors: history of bisphosphonate treatment, poor options for replacement, upcoming joint replacement surgery etc… 3)Probing depths. [Better prognosis] < 6 mm < [worse prognosis]. Deep narrow defects are a bad sign, however remember that not all teeth with fractures will present with detectable periodontal defects. 4) Radiographic findings. Is there a vertical defect or bone loss in the furcation? 5) Is the tooth vital or necrotic? There is some research to suggest that teeth that undergo necrosis from a fracture may have a poor prognosis. 6) How far apically does the crack extend internally? Good: crack stops coronal to CEJ. Questionable: Crack extends to CEJ or pulpal floor but not beyond. Poor: Crack extends into canal or onto pulpal floor. Hopeless: Crack extends entire length of tooth across pulpal floor and both margins.
2TheApex: Yes, BUT! as of Oct. 2020 it must be a REAL ID.WI, IA, and MN are REAL ID compliant states. But, your driver's license must have a gold or black star on the front to be compliant. If you don't see a punched out looking star in gold or black then time to renew or replace your license. The lines at the DMV will only get longer as the deadline approaches. You will need to bring additional documents to get the REAL ID version. It looks like a Social Security card and birth certificate or passport should be adequate for most people. Please follow links below to be sure. Mine doesn't have a star, so see you at the DMV. WI Residents IA Residents MN Residents

ToTheApex: YES!The ADA has launched a new program for finding the right person to sell your practice to OR for buying a practice. Wisconsin is one of the first states to offer it. Think of it as eHarmony for dental practices. Both owners and prospects fill out questionnaires. A real person reviews all questionnaires and matches potential practices and doctors. This is not free but I think it's really cheap considering what they are offering and other options out there.Check it out here: ADA Practice Transitions
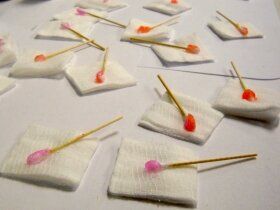
2TheApex:Yes! Our goal is to make dental visits as painless as possible. "Your comfort is our priority" can be heard daily in my operatory several times a day. Topical anesthetic is most effective for infiltration injections in areas of unattached tissue. Research does not support it's effectiveness for palatal (highly keratinized tissue) injections. But, we feel it comes down to empathy and possible placebo effect for most injection sites. The 30-60 seconds it takes to apply the topical is a trust builder with a patient we likely just met minutes earlier.How to apply it: Dry the area with a 2 x 2 gauze, place a cotton-tipped applicator with the topical at the site of future injection, cover it with the gauze and have patient close their mouth for 30-60 seconds. Then remove applicator and wipe out remaining topical with the gauze. Inject.For some injection sites it comes down to: Why Not? For the palatal injections I do skip it in favor of pressure anesthesia using the back end of my mouth mirror. Of course for some patients you may need to skip it due to allergies or medical reasons.Other tips for successful local anesthesia click here